|
|
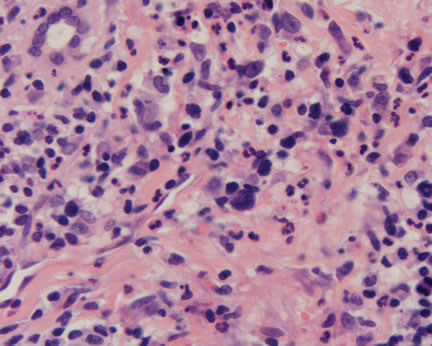
Figure 1-The characteristic atypical lymphoid cells of lymphomatoid papulosis are mixed with benign acute and chronic inflammatory cells. This histologic pattern may be mistaken for a benign inflammatory dermatosis and misdiagnosis.
|
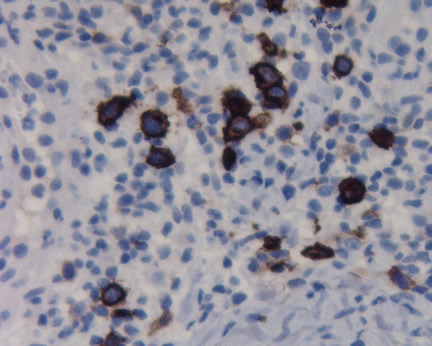
Case Study This is a 42 year old woman with diffuse papules distributed over the trunk and arms. Diagnosis: Lymphomatoid Papulosis Comment: Lymphomatoid papulosis (LyP) is characterized by recurrent papules and nodules, usually distributed over the trunk and extremities. Occasional patients may present with fewer and larger nodules. In both clinical variants, the lesions may ulcerate and become hemorrhagic. For many years, this disease was thought to be benign but contained histologically malignant cells. Currently, it is believed that this disease lies within the spectrum of cutaneous T-cell lymphomas, which includes the CD30 large cell lymphoma. Indeed, about 20% of cases may progress to cutaneous lymphomas, usually of the T-cell immunophenotype. The histopathologic features are variable and depend upon the stage of the disease. Classically, a wedge shaped infiltrate of cells is noted, distributed in a superficial and deep perivascular location. The hallmark of the disease are the atypical cells scattered throughout the benign inflammatory cells. Type A lesions usually contain numerous eosinophils and neutrophils and epidermal involvement by the atypical cells is uncommon. Type B lesions have smaller atypical cells with the nuclei having a striking hyperchromatic nucleus, sometimes referred to as chunks of coal. Epidermotropism is frequent, bearing a resemblance to mycosis fungoides. Our case (Figure 1) is best diagnosed as a Type A lesion and it is these cases that can sometimes be overlooked as a benign dermatosis. With the advent of molecular diagnostic and immunoperoxidase studies, it was found the atypical cells all express the CD30 antigen (Ki-1 antigen). (See Figure 2). This pattern is also seen in diseases as diverse as CD30+ Anaplastic lymphomas and Hodgkin's disease. Although this combination of clinical presentation and histopathology should confirm the diagnosis in the majority of cases, there have been several interesting papers in the pathology literature that have brought attention to the presence of CD30+ cells in benign inflammatory infiltrates of the skin. Surprisingly, even cases of scabies may present with these CD30+ cells! Thus, caution is always needed when making the diagnosis and correlation with the clinical appearance is recommended. All of these patients need close clinical follow-up to rule out the evolution to a malignant lymphoma. Archived Case Studies
Gallardo F, Barranco C, Toll A, Pujol RM. CD30 antigen expression in cutaneous inflammatory infiltrates of scabies: a dynamic immunophenotypic pattern that should be distinguished from lymphomatoid papulosis. The Doctor's Doctor-Skin Lymphomas The Doctor's Doctor-Mycosis Fungoides
|
Last Updated August 5, 2005
Send Emails to
Webmaster at DermpathMD
Read the Medical Disclaimer