|
|
|
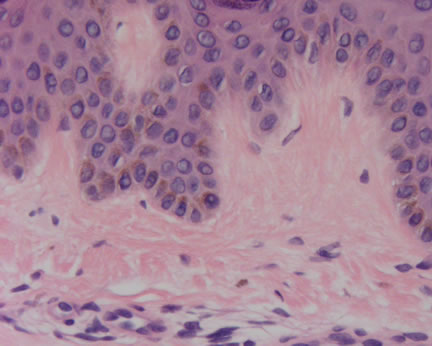
Case Study This is a 27 year old female referred by her primary care provider for uation of persistent dryness and discoloration on the right pretibial area present for approximately 2 years. Cortisone cream was prescribed with minimal change. She now presents with an approximately 6 x 10-cm area of reticulate hypo and hyperpigmentation on the right pretibial area with 2 smaller adjacent areas. Diagnosis: Comment: There are many times when the histopathologic changes are non-specific or do not appear to fit with the clinical diagnostic impression. This recent case illustrates these typical quandaries. The clinical impression was possible discoid lupus versus morphea. However, the review of the skin biopsy revealed only minimal epidermal changes resembling a lentigo. The referring dermatologist was kind enough to submit a clinical photograph with his case (see Image 2). The reticulated pattern is striking. Combining the histopathology with this clinical finding, a diagnosis of a reticulate melanotic hypermelanotic disorder is favored. In this clinical setting, Dowling-Degos disease would be a likely diagnosis. There is usually onset in early adult life, equally affecting both sexes, and may be slowly progressive. The hyperpigmentation may begin in the axillae and groin and can spread to the intergluteal and inframammary folds, neck, trunk, and arms. In our patient, a diagnosis of Reticulate Acropigmentation of Kitamura was definitely considered and indeed, there may be clinical overlap between the two disorders. In this latter disease, the reticulate changes usually initially involve the backs of the hands and then spread to other parts of the body. Onset may be during the 1-2nd decades. Palmer pits and epidermal breaks in the ridge pattern are commonly found. Several recent papers have documented an unusual association with hidradenitis suppurativa, multiple epidermal inclusion cysts, cutaneous squamous cell carcinomas and Dowling-Degos disease (see reference below). In summary, we were saved by the patient! The patient's clinical photograph prevented us from making an embarrassing and uninformed diagnosis. Thanks to the referring dermatologist for providing such a beautiful clinical photograph. References: The Doctor's Doctor-Reticulate Melanotic Hypermelanosis
|
Last Updated August 15, 2005
Send Emails to
Webmaster at DermpathMD
Read the Medical Disclaimer