|
|
|
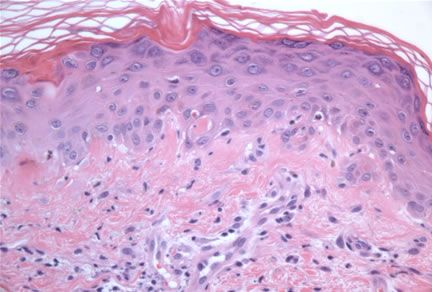
Case Study Diagnosis: Dermatomyositis Sine Myositis Sometimes a case rivets our attention because it brings to mind a recently reviewed article in the literature. This is a fascinating case of a woman who presents with a striking poikilodermatous eruption. The attending dermatologist and I considered a number of dermatologic conditions that present with poikiloderma. However, a recent paper she had reviewed presented striking clinical photos of patients who presented with a very similar rash (cited below). In this paper, the clinical diagnosis was subacute cutaneous lupus erythematosus with the patients having a variety of autoantibody profiles including a positive ANA, anti-SSA-Ro anti-SSB-La, and antithyroid microsomal antibodies. Their skin biopsies all showed an interface dermatitis with the added peculiar finding of amyloid, confirmed by immunofluorescence Thioflavin T staining. Spurred on by this fascinating differential diagnosis, I performed a Congo Red stain on the current biopsies. Alas, polarized light examination was negative for the characteristic apple-green birefringence. However, Thioflavin T is an immunofluorescence stain and is arguably a more sensitive stain for amyloid. In the United States it is not commonly utilized. Thus, the negative findings by Congo Red did not completely exclude possibility of amyloid although none of the characteristic hyalin droplets were present on routine H and E examination. The serological profile in this patient was also unusual and did not quite fit for subacute cutaneous lupus, since the majority of patients are usually ANA positive. We began to consider other diagnoses and the possibility of dermatomyositis sine myositis figured prominently. While the majority of patients with dermatomositis have a positive ANA, about 30% of dermatomyositis patients may be ANA negative but anti-SSA-Ro positive. Also dermatomyositis sine myositis patients may present with a paucity of serological abnormalities (see reference below). Further personal communication with Dr. Putnam at Beutner Laboratories in New York confirmed that "...an ANA test may be negative with patients who are Ro(SS-A) positive. Interestingly, these same patients are who are ANA negative are often C-ANA positive and Ro(SS-A) positive. Anti-Ro(SS-A) is associated with photosensitive skin rash (lupus), interstitial pneumonitis (lupus), thrombocytopenia (lupus, Sjogren's syndrome), lymphopenia (lupus, Sjogren's syndrome), nephritis (lupus), C2 complement deficiency (lupus), HLA-DQ1/2;, T-cell receptor Beta gene (lupus), vasculitis (Sjogren's syndrome), thrombocytopenia purpura (Sjogren's syndrome and SCLE), primary biliary cirrhosis." But the final nail was the removal of the patient's mascara revealing a prominent heliotrope rash (not shown because of patient identity issues). A working diagnosis of dermatomyositis sine myositis was made. The patient is being referred to a rheumatologist to evaluate for a possible myopathy. This case was satisfying on many different levels. It was a stimulating intellectual exercise to pursue a rare and unusual differential diagnosis of poikiloderma. The joy of working with a dermatologist who enthusiastically shares the clinical photos and history of their patients reminds me how exciting dermatopathology can be when it is not practiced in an information vacuum. The clinical photos and clinical information are submitted by: Elizabeth Lener, M.D.
References: The Doctor's Doctor-Dermatomyositis Caproni M, etal. Amyopathic dermatomyositis: a review by the Italian Group of Immunodermatology. Arch Dermatol. 2002 Jan;138(1):23-7. Dubois' Lupus Erythematosus,5th ed, eds Wallace DJ and Hahn BH.; chapter 25, "Antibodies to Ro(SS-A) and La(SS-B)" Harley JB and Reichlin M. 1997, Williams and Wilkins, p444. COMMENTS: |
First Posted on
June 3, 2008
Send Emails to
Webmaster at DermpathMD
Read the Medical Disclaimer